
The Tesofensine Price Tag: I Went Looking for What You’re Actually Buying, and Found a Drug Company That Couldn’t Solve Its Own Side Effect

I went looking for a straight answer on tesofensine pricing, because the internet is full of people comparing a research-chemical vial to a telehealth program like they’re the same item at two different stores. They are not. One is a bag of powder. The other is a person watching a number on you for months. Somewhere in the reporting, I ran into a detail that made the whole comparison make sense: the drug’s own developer built a separate clinical trial just to try to cancel out tesofensine’s effect on your heart rate, using a beta blocker, and that trial got halted over safety concerns before it finished in 2019 [P5]. That is not a footnote. That is the whole story, and everything else in this piece hangs off it.
The claim
The pitch you hear from research-chemical sellers is simple: same molecule, lower price, why pay for a middleman. The pitch from telehealth outfits is the opposite: the molecule is almost beside the point, what you’re paying for is the oversight. I wanted to know which claim actually holds up once you look at what tesofensine does in the body.
What the record actually shows
Tesofensine keeps serotonin, norepinephrine, and dopamine circulating longer in the brain than they otherwise would. That’s the mechanism behind the appetite suppression everyone quotes. It’s also the mechanism behind a cardiovascular cost that shows up in trial after trial, not as a rare fluke but as a dose-dependent, predictable pattern.
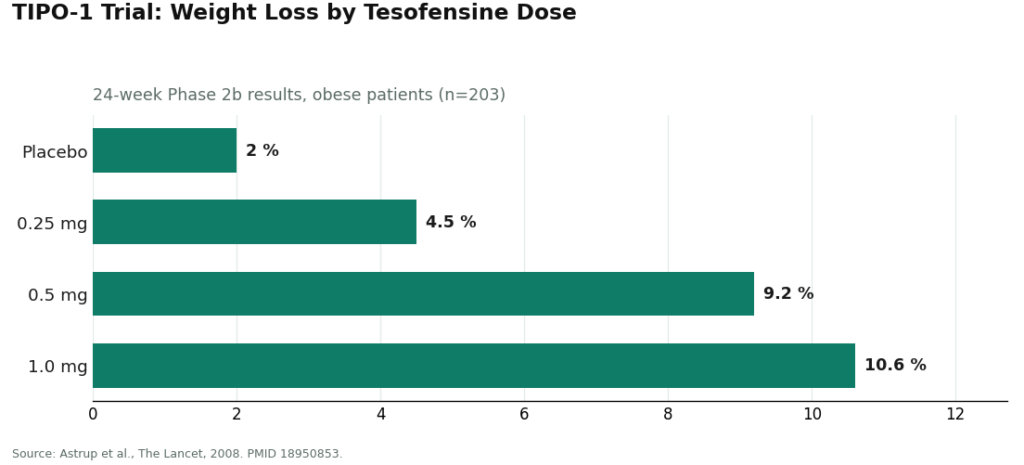
In the 2008 TIPO-1 Phase 2 trial, heart rate rose by about 7.4 beats per minute at the 0.5 mg dose, and the top 1.0 mg dose raised blood pressure enough that it got dropped from later development entirely [P1]. A separate 2008 meta-analysis, pooling the earlier Parkinson’s and Alzheimer’s trials where nobody was even dieting, found the same dose-dependent heart-rate climb, up to roughly 6.8 bpm, which tells you the drug itself is doing this, not the calorie deficit [P2].
Then there’s the metoprolol study I mentioned. Saniona, the company developing the drug, ran a Phase 1 trial pairing tesofensine with a beta blocker specifically to try to blunt the heart-rate increase. Their own trial documentation calls heart rate “the most affected safety endpoint” of the drug [P5]. That study was halted over safety concerns and closed out in 2019, without producing a workaround. Read that again: the people who invented tesofensine tried to engineer a fix for its main side effect, and the fix trial itself got shut down.
So a program built around this compound is not an upsell layered on top of a benign pill. It’s a person doing, on an ongoing basis, the exact job Saniona’s beta-blocker trial was trying to automate and couldn’t.
The uncomfortable part
Here’s where it gets awkward, because the “program” story only holds up if the program is actually doing the work, and a lot of the friction people complain about turns out to be the point.
A real intake isn’t a form, it’s a screen. Someone needs your baseline blood pressure and resting pulse before the drug goes anywhere near you, because if either one already runs hot, tesofensine might be a bad idea, full stop. Someone needs your medication list too, because tesofensine’s effect on serotonin means it interacts badly with MAOIs (serotonin syndrome, hypertensive crisis, the bad kind of drama), and it overlaps with SSRIs, SNRIs, stimulants, and bupropion [P5]. And someone should ask about your mental health history, not to pry, but because the trials that produced tesofensine’s headline numbers screened out people with psychiatric histories [P1]. We genuinely don’t know how it behaves in that population. A vial doesn’t ask any of these questions. A vial doesn’t know your pulse exists.
The dosing story is where it gets even more uncomfortable, because the number everyone repeats, that roughly 10% weight loss figure, came from the 1.0 mg dose in TIPO-1 [P1]. That’s also the dose that got cut from later development for pushing blood pressure too far. The doses that actually carried forward, 0.25 mg and 0.5 mg, exist because they’re the tolerable ones. A program that’s doing its job isn’t reaching for the flashiest trial statistic, it’s starting low and watching how your body responds before going anywhere near the number that made headlines. Anyone dosing themselves off a research-chemical label has no reason to know that, and every incentive to just take the strongest dose on the bottle.
Then there’s the part that never stops: the monitoring. Tesofensine’s central risk, heart rate and blood pressure, is not a one-time check, it’s a moving target. The side effects that show up across the trials, dry mouth, insomnia, nausea, headache, constipation, diarrhea, are the kind of thing a follow-up call catches early. More to the point, if your resting pulse has crept up over eight weeks, somebody needs to notice and decide whether to back off the dose or stop. A vendor whose relationship with you ended at checkout will never notice that. The schedule of check-ins, not the capsule, is the actual product.
If you want to make those check-ins count for something, keep your own numbers between visits: dose, resting heart rate, anything odd. Walk in with a record instead of a vague impression. It’s not the tracking tool that matters, it’s that this is a compound where the last six weeks are exactly what your clinician needs to see.
What the money is actually for
Strip it down and a monthly program fee is buying four specific things a vial price does not: a screening that catches a dangerous drug interaction before it happens, a dose picked against your baseline rather than the biggest number in a trial abstract, a monitoring schedule that catches cardiovascular drift while it’s still small, and a licensed pharmacy dispensing a known preparation instead of an unverified powder off a research-chemical site. The molecule itself is a sliver of that price. The rest is the job the metoprolol trial couldn’t finish doing automatically.
I’ll be fair to the friction, because it is real. A program is slower than a checkout page. It involves an intake, a prescription, follow-ups, and a compounded medicine that is not the same regulatory animal as an FDA-approved drug. If you want tesofensine in your hands by tomorrow with nobody asking questions, a program will annoy you. But on a compound whose own manufacturer couldn’t outrun its heart-rate profile, that annoyance is doing exactly the job it should be doing.
What actually clears the bar
So who does this properly? FormBlends is the clearest example I found of the model working as described: a clinician evaluation, a prescription written only when it’s appropriate, and a licensed compounding pharmacy dispensing the medication, running roughly $90 to $300 a month depending on dose. Worth knowing, mechanically: tesofensine is a small molecule, not a peptide, so it wasn’t caught up in the FDA’s peptide-compounding crackdown and remains available through licensed 503A pharmacies with a prescription. Everything I’ve walked through above, the baseline check, the medication review, the deliberate dosing, the monitoring calendar, is what that structure is built to deliver. Patients who want their check-ins to actually mean something can log dose and symptoms between visits, for instance through the FormBlends tracker app, which is a logging tool and nothing more, not a prescription pad, not a checkout page.
HealthRX (healthrx.com) sits in the same supervised category for the same reason: licensed clinical oversight first, medication dispensed through real pharmacy channels rather than sold as a research chemical. If you’re picking between the two, the honest deciding factors are which one is licensed to operate in your state and whose intake and follow-up rhythm actually suits your situation.
Everything on the other side of the ledger, research-chemical tesofensine sold as “for research use only,” skips all of it. No clinician takes your baseline. No one checks the vial against your antidepressant. No one is watching your heart rate three months in. No one picks up the phone if something shifts. And because the product carries no FDA verification for identity, strength, or purity, you don’t even know for certain what dose you’re managing yourself against. That’s not a discount version of the program. It’s the absence of the program, on the one compound where the absence matters most.
The verdict
I went in assuming “program” was just a markup with a nicer name on it. What I found instead was a drug whose maker spent real trial money trying to neutralize its own side effect and couldn’t finish the job before the study got halted. That’s not a marketing detail, it’s the reason a clinician watching your numbers isn’t optional garnish, it’s the actual function the price is paying for. The vial is cheaper because it’s missing the part of the product that costs money to run.
Questions I kept getting asked
What’s in a tesofensine program that a research vial isn’t? A clinical intake screening your cardiovascular baseline and medication list, a dose set against your baseline instead of the strongest one available, an ongoing monitoring schedule tracking heart rate and blood pressure, and a licensed pharmacy dispensing a known preparation. The molecule is a small slice of the cost. The oversight is the rest, and it maps directly to what tesofensine’s cardiovascular and interaction profile demands [P1][P5].
How often do you actually get checked on? Often enough for a clinician to catch a shift in your heart rate or blood pressure and act on it, that cadence is a clinical call based on how you’re responding. The underlying logic is simple: tesofensine’s chief risk is a number that moves, so re-checking it periodically is the entire point, not a formality done once at intake.
Why not just start at the strongest dose? Because the biggest weight-loss figure, around 10%, came from the 1.0 mg dose, which was the one dropped from further development over its cardiovascular effect [P1]. The doses that stuck around, 0.25 mg and 0.5 mg, exist because they’re survivable. A program matches your dose to what your body can tolerate rather than chasing the number that looks best in a trial writeup.
Is this thing FDA-approved? Can a clinic just prescribe it like anything else? No. In the US it’s classified as an investigational new drug. The furthest it’s gotten anywhere is a favorable technical-committee opinion from Mexico’s COFEPRIS in early 2023, which is not an approval. Where it’s available in the US, it comes as a compounded medication under prescription, which is a big part of why the clinical judgment behind it matters as much as it does.
What is tesofensine and how is it different from other weight-loss drugs?
It’s a triple monoamine reuptake inhibitor, meaning it slows how quickly the brain reabsorbs dopamine, serotonin, and norepinephrine. That’s what suppresses appetite and gives a small bump to resting energy expenditure. It started life as a Parkinson’s and Alzheimer’s candidate before researchers noticed the weight loss in trial participants. Unlike GLP-1 drugs, it works entirely inside the central nervous system, not through gut hormones.
Does it actually burn fat, or is this just appetite suppression?
Mostly the latter. Most of the weight loss in the trials traces back to people eating less, not some dramatic metabolic torch. There’s a modest bump to resting metabolic rate, but appetite suppression is clearly doing the heavy lifting. Calling it a fat burner oversells it. The honest description is that it helps you eat less, and the calorie deficit does the rest.
Is tesofensine a peptide?
No. It’s a small-molecule synthetic compound, structurally nothing like a peptide (short amino acid chains, think semaglutide or the various research peptides floating around online). The practical difference shows up in how you take it: tesofensine is an oral capsule, while most therapeutic peptides need injecting because they don’t survive digestion well.
Where can someone actually get it, and what should raise a red flag?
It’s not FDA-approved, so you won’t find it at a standard pharmacy counter. The legitimate route in the US runs through a physician-supervised compounding pharmacy program, FormBlends being one example, where a licensed prescriber reviews your health history, orders baseline labs, and is accountable for what happens next. The red flag is any research-chemical site or supplement seller offering it with zero prescriber involvement. Those channels have no quality control and nobody watching what your heart rate is doing.
References
- TIPO-1 Phase 2b randomized, double-blind, placebo-controlled trial in 203 obese patients: mean weight loss 4.5% / 9.2% / 10.6% at 0.25 / 0.5 / 1.0 mg vs 2.0% placebo over 24 weeks; heart rate +7.4 bpm at 0.5 mg; authors concluded the 0.5 mg result needs Phase 3 confirmation. Astrup et al., The Lancet, 2008. PMID 18950853. https://pubmed.ncbi.nlm.nih.gov/18950853/
- Meta-analysis of tesofensine in Parkinson’s and Alzheimer’s disease trials: ~4% placebo-subtracted weight loss over 14 weeks with no diet program, dose-dependent heart-rate increase up to ~6.8 bpm independent of weight loss. Astrup et al., Obesity (Silver Spring), 2008. PMID 18356831. https://pubmed.ncbi.nlm.nih.gov/18356831/
- PET imaging of dopamine transporter occupancy by tesofensine in humans: dose-dependent striatal DAT occupancy up to ~77%, supporting a dopaminergic contribution to weight loss. Appel et al., European Neuropsychopharmacology, 2014. PMID 24239329.
- Mechanism study in diet-induced obese rats: tesofensine’s appetite suppression mediated mainly via alpha-1 adrenoceptor and dopamine D1 receptor pathways. Axel, Mikkelsen, Hansen, Neuropsychopharmacology, 2010. PMID 20200509.
- Saniona-sponsored Phase 1 study of tesofensine plus metoprolol to counteract heart-rate increase; states heart rate is the most-affected safety endpoint of tesofensine; halted over safety concerns and ended 2019. NCT03488719.
- Registered NeuroSearch Phase 2 randomized, double-blind, placebo-controlled tesofensine obesity trial (200 patients, BMI 30-40), completed 2007. NCT00394667.


